Guidelines SOSORT 2016: Physiotherapy & Sport
Principles are guidelines for human conduct that are proven to have enduring, permanent value.
Stephen Covey
 |
Two centuries ago, the inaugural book dedicated to exercises specifically targeting scoliosis was published, laying the groundwork for what is now known as the Lyon Method. In the realm of physiotherapy, whether integrated with bracing or surgical interventions, European advancements have given rise to a multitude of validated approaches. Despite their diversity, these methods are unified by foundational principles that underpin this chapter. The primary objective across all techniques is to curtail the progression of scoliosis. Once the extent of vertebral deviation is assessed, the patient is instructed in three-dimensional correction of the spinal curvature, with a strong consensus focusing on geometrical detorsion combined with active axial self-elongation. This corrective action is to be sustained throughout daily activities, regardless of whether a brace is employed. Whether varied in execution, respiratory techniques invariably serve as a complement to spinal exercises.
|
 |
From the onset of the chaotic phase, physiotherapy should be employed as a primary defense mechanism. During the crucial growth phase, the primary objective is to curb the advancement of scoliosis and, for more pronounced curvatures, reduce reliance on braces. However, assessing the efficacy of this physiotherapy presents challenges, as predicting the trajectory of scoliosis in each individual child remains difficult. In numerous countries, there is a scarcity of physiotherapy resources. This scarcity raises the concern of imposing costly and potentially burdensome physiotherapy on a child whose scoliosis might not progress. Should progression occur, physiotherapy not only proves effective on its own but also amplifies the mechanical benefits of wearing a brace
|
 |
Scoliosis-specific physiotherapy exercises are developed through an agreement among various validated approaches. The strongest agreement centers on assessing and mastering the 3D self-correction of spinal curves. This correction must be sustained throughout daily activities, a practice referred to as the "24-hour back care" in the Lyon Method. The concept of therapeutic patient education, though more contemporary, plays an integral role in the learning process during growth phases. Advancements in technology provide easier access to information, which therapists should leverage to promote the consistent practice of exercises at home, thereby enhancing adherence to the prescribed treatment.
|
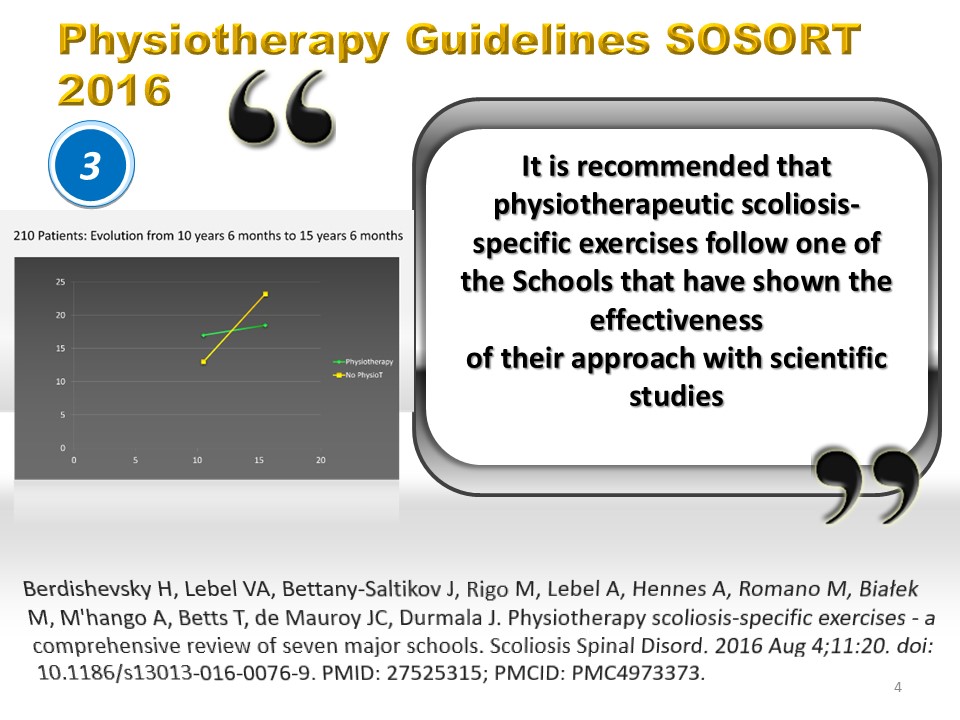 |
Numerous techniques have been substantiated through rigorous scientific research. Many of these practices also draw on centuries-old wisdom. However, validating these methods presents challenges, particularly because parents are often reluctant to engage in randomized studies. Furthermore, distinguishing the impact of physical exercise from the influence of a patient’s personal motivation can be quite complex. The Lyon Method underwent validation in this challenging context by two concurrent research teams. For angles between 15° and 25°, the decision to randomize was made by the attending physician. When physiotherapy was prescribed, it was administered regularly, while the other group continued to undergo systematic observation. The progression of those receiving physiotherapy, illustrated in green, between the ages of 10 and 15, showed a statistically significant divergence from the evolution of those without physiotherapy, depicted in yellow.
|
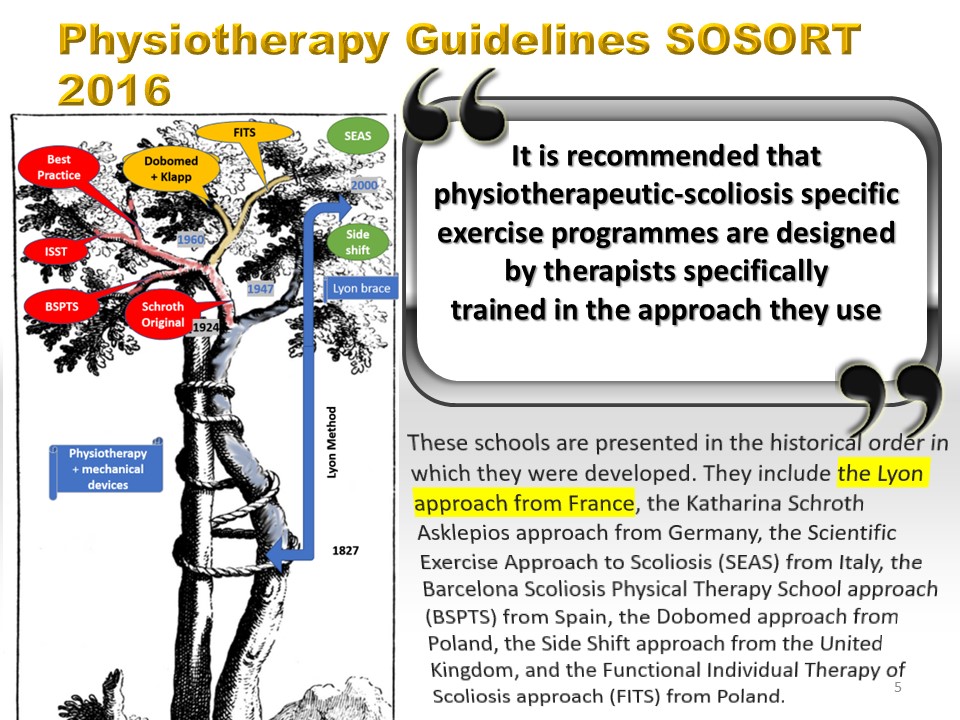 |
Numerous educational institutions provide supplementary training in these techniques, which, regrettably, are not consistently incorporated into standard university curricula. These institutions are introduced in the chronological sequence of their development. This includes the Lyon method originating from France, the Katharina Schroth Asklepios method from Germany, Italy's Scientific Exercise Approach to Scoliosis (SEAS), Spain's Barcelona Scoliosis Physical Therapy School approach (BSPTS), Poland's Dobomed method, the Side Shift method from the United Kingdom, and Poland's Functional Individual Therapy of Scoliosis method (FITS). More recently, the Klapp method has gained formal validation.
|
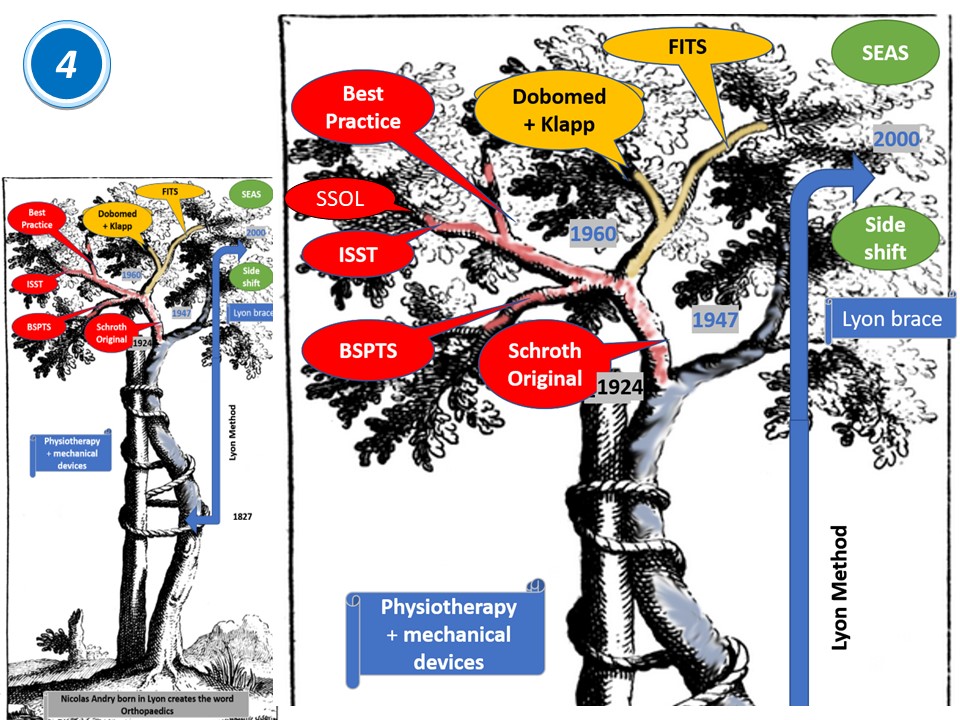 |
These various techniques can be categorized into distinct groups. Highlighted in red are several schools that emphasize the Schroth method: Germany's renowned International Schroth Three Dimensional Scoliosis Therapy, the innovative Barcelona school, Weiss' Best Practice approach, and the Canadian school led by Lebel. Marked in orange are the Polish methodologies: Dobomed, which is a synthesis of the Schroth and Klapp techniques, and FITS, a method incorporating resistance bands. In green, we find two approaches that concentrate on specific components of Physiotherapeutic Scoliosis Specific Exercises (PSSE). The side shift technique primarily employs translation movements in the frontal plane, whereas SEAS emphasizes cortical three-dimensional correction. While the original intention of the Schroth method was to eliminate the necessity for a brace, it is observed that all European physiotherapy schools advocate the use of a brace in practice. The Chêneau brace is recommended for the Schroth method, whereas more rigid braces are favored for both the Lyon Method and SEAS.
|
 |
Numerous techniques have emerged within dedicated scoliosis treatment centers, where an interdisciplinary team comprising doctors, ortho-prosthetists, and physiotherapists is available. Such a specialized center ensures that all practitioners collaborate closely, unified by a common understanding and approach to the patient’s care. In contrast, within a hospital environment prioritizing a technical platform, the onus falls on the patient to navigate from one specialized department to another, complicating the seamless collaboration among healthcare professionals. A further significant benefit of such specialized centers is that they enhance the educational experience for students, as they have the opportunity to learn from a concentration of patients with similar conditions. Moreover, bringing patients together in these settings fosters dialogue among them and their families, which, in turn, enhances treatment adherence.
|
 |
The diverse nature of scoliosis necessitates a personalized approach to treatment, carefully considering the patient’s unique circumstances, the specific curvature type, and the current stage of therapy. Within the Lyon Method, there exists a carefully devised set of 12 foundational exercises. These exercises are strategically grouped to ensure a seamless progression, not only within each session but also across the prescribed 30 sessions and the entirety of the treatment process. Each exercise has been thoughtfully designed to accommodate the development level of the postural system, the flexibility or stiffness of the vertebral muscles, and the susceptibility to fatigue or overactivity of the muscular system.
|
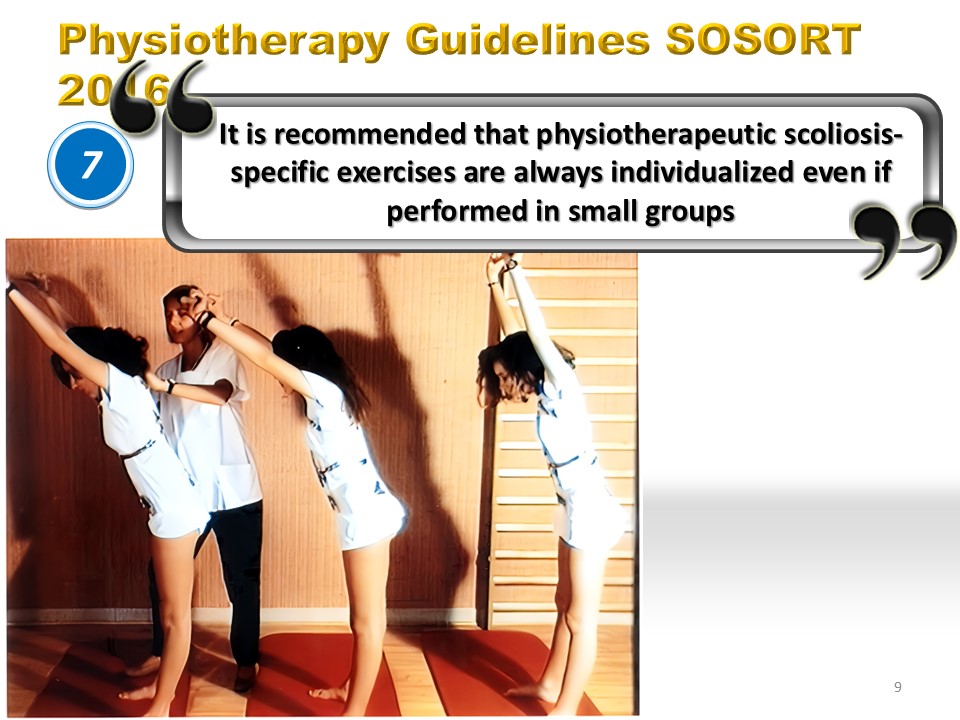 |
Engaging in small group exercises significantly enhances stimulation for children, particularly when it comes to exercises numbered 5-6 and 9-12. Gathering patients in specialized centers, such as during the distribution of braces, facilitates a sense of community and togetherness. Moreover, integrating a technical procedure with a physiotherapy session can be quite beneficial. For instance, before molding begins, a session may include relaxation techniques and a reassessment of corrected postures. During the delivery of the brace, exercises focused on maintaining proper sitting posture and mastering the "grand porter" move can be incorporated. Furthermore, ballistic stretching exercises are recommended when the brace is being evaluated for adjustments.
|
 |
Upon the initial diagnosis of scoliosis, physiotherapy emerges as a crucial component of treatment. This remains true even as the treatment concludes, particularly when the patient transitions away from using a brace. Throughout the various stages of growth, scoliosis-specific exercises can be tailored to fit each phase, ensuring they serve as a constant aid. To prevent the patient from losing interest and to guard against the abandonment of the regimen, it is vital that these exercises are diversified and engaging. Within the framework of the Lyon Method, these exercises play a supportive role alongside regular sports activities, fostering long-term commitment in the child. Adding an element of enjoyment, these exercises can also be fashioned into a form of specialized sports training, making the experience both beneficial and enjoyable.
|
 |
One significant benefit of physiotherapy during the treatment process is the consistent schedule of weekly sessions, which is crucial for a child who naturally focuses on the present moment. The effectiveness of practicing exercises at home can be monitored by maintaining a daily journal. Nowadays, several mobile applications are available that facilitate the tracking of scoliosis progression, with some utilizing artificial intelligence to enhance posture based on photographic analysis. Nonetheless, it's important to ensure that these interventions do not overly disrupt the child's daily routine or evoke feelings of guilt.
|
 |
Typically, the physiotherapist makes adjustments to the exercise regimen on a weekly basis, and it is imperative for the child to diligently practice these exercises at home each day. Nevertheless, it is crucial to scrutinize the quality of these exercises to prevent issues such as the development of counter-curves. Within the framework of the Lyon Method, maintaining the alignment of the head along the line of gravity is essential to ensure the correct positioning of the semicircular canals. Additionally, it is vital that the pelvis is properly aligned, avoiding any asymmetry in the lower limbs. Thoracic bending should occur between T2 and T10, ensuring that no counter-curvature arises at the lumbar region.
|
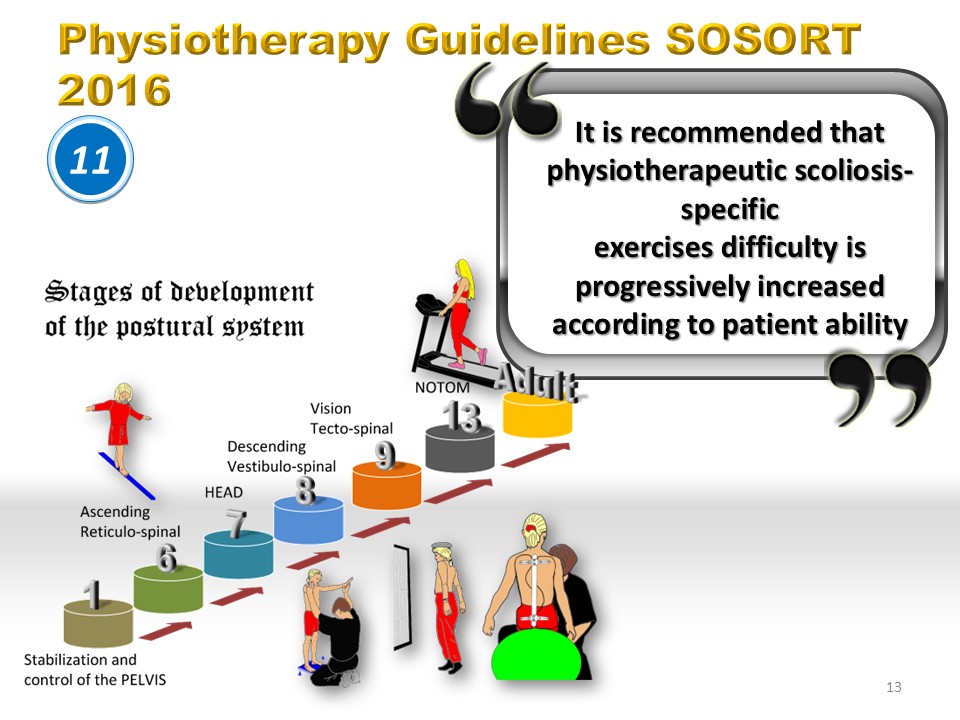 |
The development of the vertebral postural system continues until a child reaches the age of 12, necessitating that any stimulation for younger children should consider this ongoing growth. In cases of idiopathic scoliosis, the notion of Neuro Osseous Timing Of Maturation (NOTOM) is significant. This concept, which involves a delay in the development of the postural system in comparison to bone growth, sheds light on why idiopathic scoliosis is more common in girls than in boys. By the age of 7, children typically have the ability to walk steadily across a beam 5 cm in width without losing balance. When they reach 8 years old, they can accurately throw a ball to hit the center of a target. By the age of 9, the child has acquired a complete body schema. As they progress to 10 or 11 years old, they begin to hone their precision and speed. By the age of 12, their agility and coordination are fully developed, marking the maturation of the postural system. During the pubescent years, children further develop endurance, strength, stamina, and power.
|
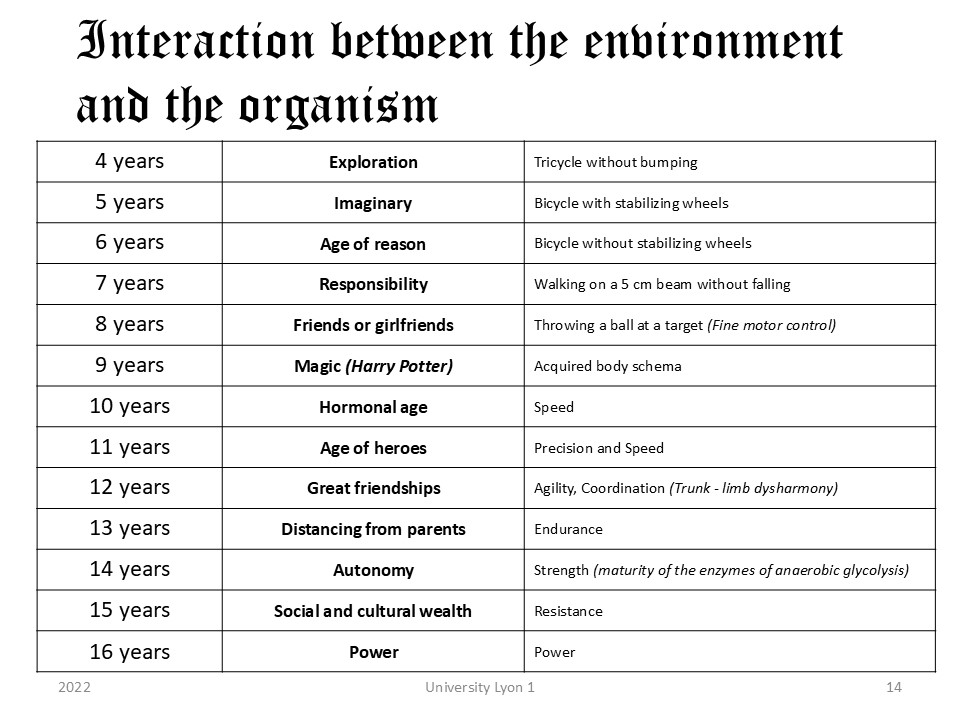 |
As individuals grow older, their psychological environment matures alongside their physical development. A child should not be viewed simply as a small version of an adult. Initially, during a period of spatial exploration, a child's environment is largely shaped by imagination and creativity. Over time, this imaginary world begins to intertwine with the realities of everyday life. During this transformation, children often find companionship with peers, sharing a whimsical realm filled with heroic figures and fantastical adventures. However, the onset of puberty signals the end of this enchanting era, ushering them towards the adult world. In this new phase, the young person navigates life with social and cultural norms that differ from those of their parents. They move towards independence, equipped with the formidable tools of modern technology.
|
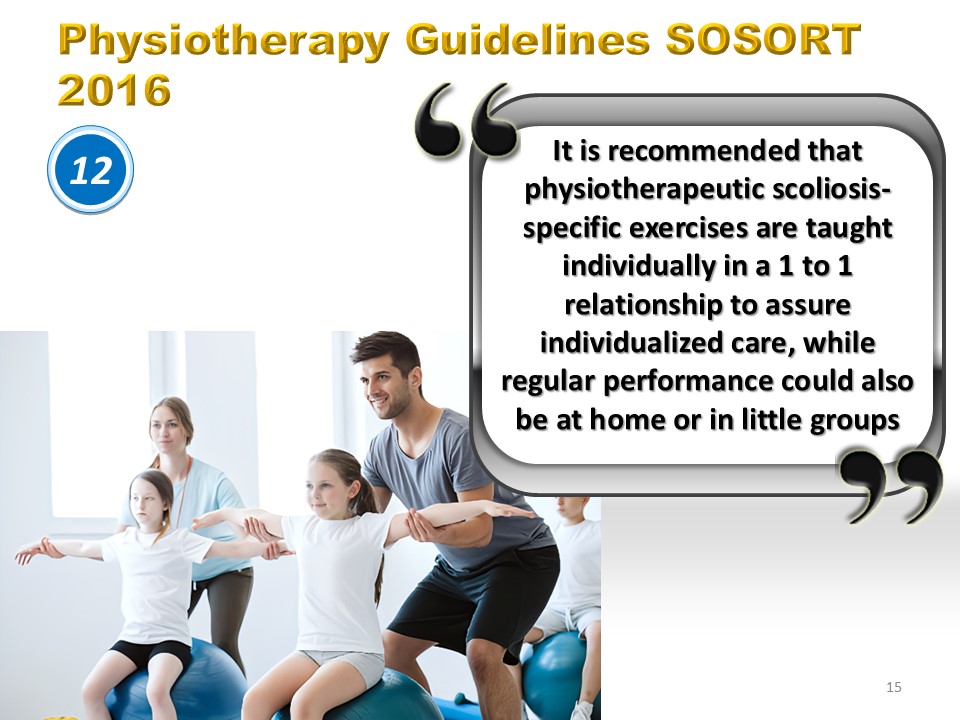 |
When an exercise is tailored specifically for a child, it can be easily practiced at home with minimal equipment. The most beneficial tools in this regard are a mirror and a Swiss ball. Within this framework, it is feasible to conduct activities involving small groups of children of a similar age, thereby considering the development of their postural systems.
|
 |
Wearing a brace serves not as a substitute for physiotherapy, but as an enhancement to it. The integration of a brace with physiotherapy forms the cornerstone of the Lyon Method. Specifically, exercises numbered 9, 10, and 11 are designed to recalibrate the postural receptors, which are responsive to stretching and movement, ensuring they adopt a perfectly corrected stance. Consistent physiotherapy plays a crucial role in organizing the child's daily routines and fosters better adherence to the treatment plan.
|
 |
Interestingly, the early stage of wearing a brace full-time is advantageous for gradually adjusting to it, according to the watch principle. Continuous contact with the skin alters its sensitivity over time. After overcoming the initial self-conscious phase, where the child feels the gaze of others, the brace begins to serve as a form of protective armor during the challenging adolescent years. It is the physiotherapist who is ideally equipped to guide the child through this transitional phase. The duration of treatment is extensive, and it is crucial not to discontinue it until the bone density is sufficient to endure the excessive stress caused by scoliosis. Engaging in sports can frequently lessen the need for as many physiotherapy sessions. However, the period of gradually discontinuing the brace is often quite sensitive, as the child may feel the loss of its protective barrier.
|
 |
Physiotherapy, while beneficial, may not always eliminate the necessity for a brace, particularly when considering bone fragility and the concept known as Ian Stokes' vicious circle. From a physiological standpoint, the bodily structures exhibit elasticity within the frontal plane, and it is the brace that offers the requisite plastic correction. For the brace to function optimally, it is essential that the correction is most pronounced at the curve's apex. Moreover, within the framework of the Lyon Method, the adjustment is performed directly on the patient and can be repeated prior to the molding process. On this picture, it is crucial to give special attention to the alignment of the lower limbs to effectively widen the ilio-lumbar angle at the level of the left convexity.
|
 |
During the weaning phase, self-corrective exercises are persistently practiced. At this stage, the muscles need to take over the responsibility of the brace to uphold the correction of the curve. Initially, these exercises are conducted while on all fours, then progressed to a seated posture, and finally, executed in a standing stance. The corrected posture is held steadily for a duration of 20 seconds.
|
 |
Similar to wearing a brace, undergoing surgery does not signify the conclusion of physiotherapy. Even though modern surgical methods are minimally invasive, the recovery phase can be quite painful. Physiotherapy plays a crucial role in this period by alleviating the discomfort of scar tissue and facilitating the development of compensatory mechanisms both above and below the site of arthrodesis.
|
 |
The type 1 slow-twitch muscle fibers within the extrapyramidal postural system primarily operate through aerobic processes. Furthermore, it’s important to note that in cases of scoliosis, type 2 pyramidal fibers do not experience any significant deficiency. As a result, anaerobic resistance training is rarely employed. Instead, greater focus is directed towards enhancing the flexibility of non-arthrodesed curves.
|
 |
Functional respiratory limitation becomes notably significant when the thoracic curve exceeds 70 degrees. However, it's worth mentioning that even at smaller angles, individuals may experience respiratory limitations during rigorous physical activities. Additionally, the use of braces can further restrict vital capacity. Within the framework of the Lyon Method, directing one's breathing towards the concavity of the curve is not deemed crucial. This is because thoracic bending, in contrast to thoracic translation, actually increases the concavity's volume. The primary focus, therefore, is placed on enhancing the mobilization of the expiratory reserve volume.
|
 |
Donning a brace modifies the interaction between the spine and the diaphragm, integral components of the deep front line. This alteration can impede the growth of the ribcage and lungs, especially concerning infantile scoliosis and symmetrical braces. Therefore, it is crucial to closely supervise the renewal of the brace. When engaging in physical activity, it is most effective to address flat backs and scoliotic curvatures during the phase of exhalation. Additionally, it has been observed that to enhance postural musculature, one should focus on aerobic metabolism, which essentially involves optimized breathing techniques.
|
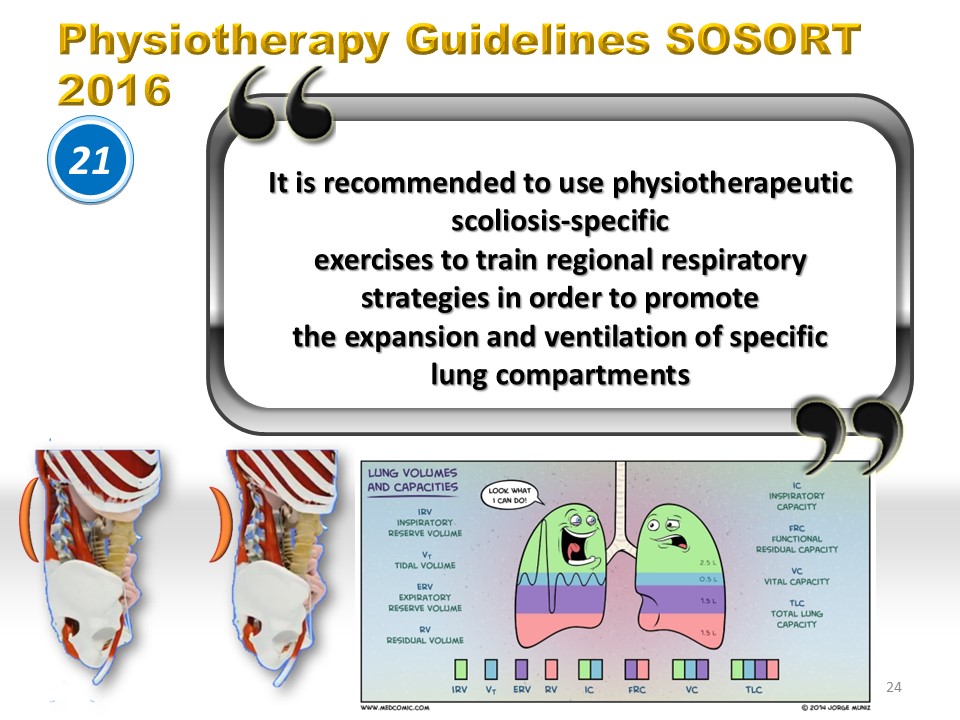 |
Scoliosis correction is typically addressed above the T10 vertebra through the ribs, which frequently become more upright in the area of convexity. Asymmetrical braces provide the benefit of allowing for expansion into the concave side, in contrast to symmetrical braces, which do not offer such flexibility. For effective high thoracic respiration, it is essential to maintain mobility in the sternoclavicular area. Below the T10 level, the transfer of soft tissue can impede abdominal breathing, particularly when it is executed in a corrected lordosis position. Although corrected lordosis can enhance sagittal push-up capabilities, it concurrently restricts the ability for abdominal breathing.
|
 |
The discussion surrounding the involvement of sports in managing scoliosis remains a topic of intense debate. In the context of the Lyon Method, athletic activities have consistently served as a valuable supplement to targeted exercises. Regarding the postural system, engaging in sports not only encourages anticipation but also significantly enhances functionality, particularly in terms of endurance. Intriguingly, even when adolescents participate in asymmetrical sports, there is no statistical link to the progression of scoliosis, potentially supporting the rationale for brace utilization. Furthermore, in adulthood, maintaining a routine of regular physical activity contributes to the preservation of stability.
|
 |
Engaging in sports plays a vital role in enhancing the postural system, yet it should not be mistaken as a targeted remedy for scoliosis. The three-dimensional curvature of the spine remains unaltered by sports activities. Furthermore, while a physiotherapist relies on feedback mechanisms to correct posture, sports inherently promote anticipation. Initially, individuals focus on developing advanced motor skills such as walking. Activities like cycling, whether with stabilizers or without, are instrumental in fostering balance. As adolescents progress through puberty, they can participate in a wide array of sports. Once they reach the conclusion of their growth spurts, the axial force exerted during running generates a piezoelectric effect. This effect facilitates the fixation of calcium along the spine, subsequently enhancing bone density.
|
 |
Engaging in sports activities fosters an array of psychological benefits, such as boosting self-assurance, nurturing independence, enhancing decision-making skills, and encouraging the development of mutual support among individuals. For children with an abundance of energy, sports provide a valuable outlet for releasing surplus vigor while simultaneously cultivating self-discipline. Moreover, participating in sports enhances one's ability to focus and concentrate, alongside augmenting other cognitive functions. The positive impact extends to promoting better sleep quality and increasing melatonin production. Furthermore, engaging in sports contributes to harmonious physical development, aiding in the maintenance of an optimal body weight, while also enhancing flexibility and balance.
|
 |
Participation in school sports activities is generally encouraged, except in cases where a brace is worn on a permanent basis. This is primarily because the brace restricts trunk mobility and poses potential risks to others during contact sports. One of the most common limitations involves the handling aspect in acrosport, which has the potential to exacerbate bone deformation. According to the Lyon Method, the time allocated for daily removal of the brace does not account for the hours dedicated to engaging in sports. The axial muscles function similarly to an active brace, helping to reduce the deformation of the vertebral body.
|
 |
In specialized centers, individuals engage in sports activities while wearing the brace during the initial phase of acclimatization. The advantages are numerous and significant. Firstly, there is a reprogramming of postural receptors to align with the corrected position. Secondly, all the advantages associated with sports activities are preserved. Lastly, there is an enhancement in athletic performance when maintaining the corrected posture.
|
 |
Engaging in combat sports fosters the enhancement of coordination, balance, respect, discipline, and self-assurance, while also encouraging the cultivation of beneficial habits. From a physical standpoint, these activities contribute significantly to building endurance, strength, and flexibility. Yet, despite these advantages, pediatricians generally advise against boxing for children. The rigorous nature of this sport can present challenges during the developmental years. Repetitive micro-traumas incurred from intense training may result in spondylolysis, which, alarmingly, is linked to lumbar scoliosis in 20% of the cases.
|
 |
Engaging in sports that demand significant bending or stretching of the spine—like gymnastics, dance, and certain types of yoga—can often result in the loosening or compressing of the vertebrae. The ligaments play a crucial role in safeguarding the joint system; however, there's a potential danger of disrupting the Tensegrity, which is essential for maintaining the stability required in high-level athletic activities.
|
 |
In summary, the SOSORT guidelines encapsulate nearly two centuries of accumulated knowledge in the orthopedic treatment of scoliosis. Despite the evident variety in approaches, there exists a broad agreement on the methods involving physiotherapy and bracing. This diversity allows for a more tailored approach in addressing the varied manifestations of scoliosis, all while adhering to the established guidelines. The 68 guidelines have been thoroughly illustrated and discussed in this dual presentation, providing a comprehensive roadmap for the ongoing journey in scoliosis management.
|
|
|
To register for Certification, please contact SSOL
|


