17.9 Decision tables & Decision trees
 |
For over two hundred years, the Lyon method has been a harmonious blend of bracing and physiotherapeutic techniques aimed at halting the progression of scoliosis and thus reducing the necessity for surgical intervention. In cases of idiopathic scoliosis, the therapeutic strategy emerges from a multitude of compromises, primarily influenced by the degree of spinal curvature, the specific area of the spine affected, and the age of the patient. This strategy is not only the culmination of extensive experience but also is supported by evidence derived from successful outcomes. While inevitable adjustments must be made in response to advancements in technology and shifts in the environment, these modifications remain relatively minor. The fundamental principles of the approach have been derived from the SOSORT guidelines. |
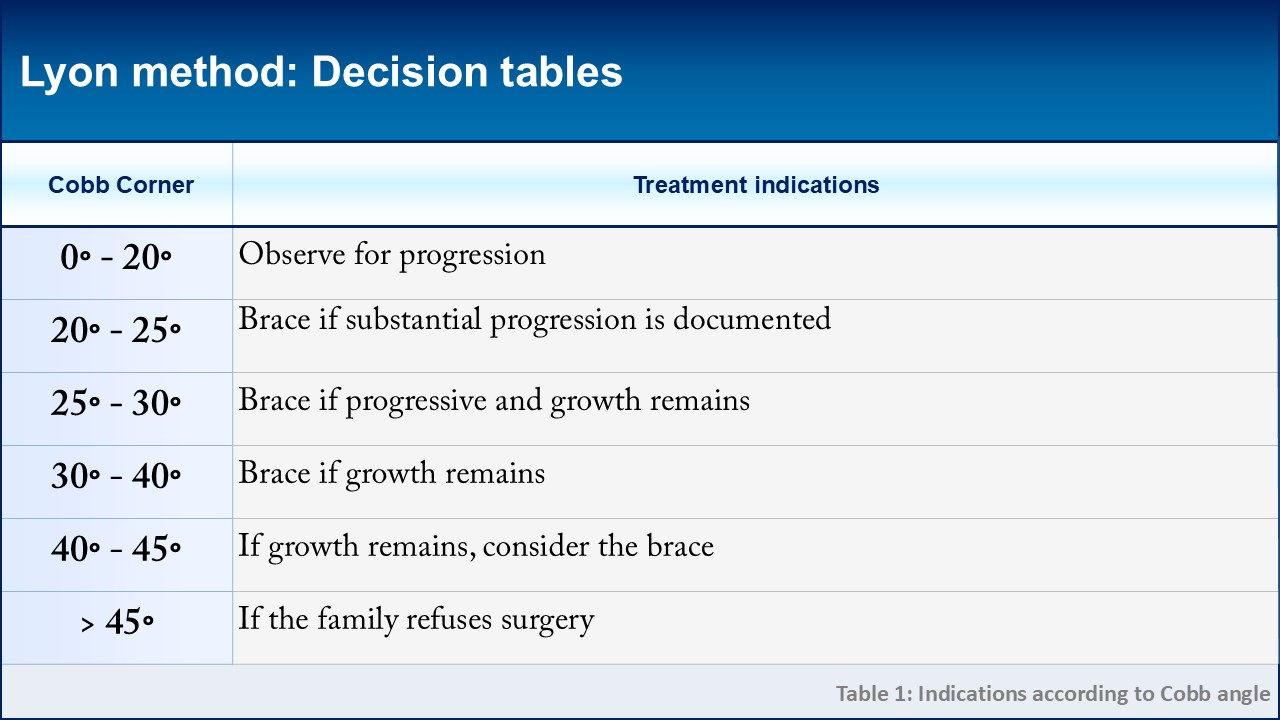 |
The Cobb angle measurement continues to be regarded as the "gold standard" in determining therapeutic indications for scoliosis, even with the inherent inaccuracies of a frontal plane projection. Remarkably, the primary criteria for these indications have remained largely unchanged for over half a century. Nonetheless, the concept of growth invites further discussion. In contemporary practice, greater emphasis is placed on bone mass rather than growth alone, as bone mass peaks following the cessation of growth and significantly influences the strength of the vertebral body. Consequently, the Lyon method opts to address scoliosis post-Risser 3, incorporating a gradual reduction of brace wear towards the conclusion of treatment. |
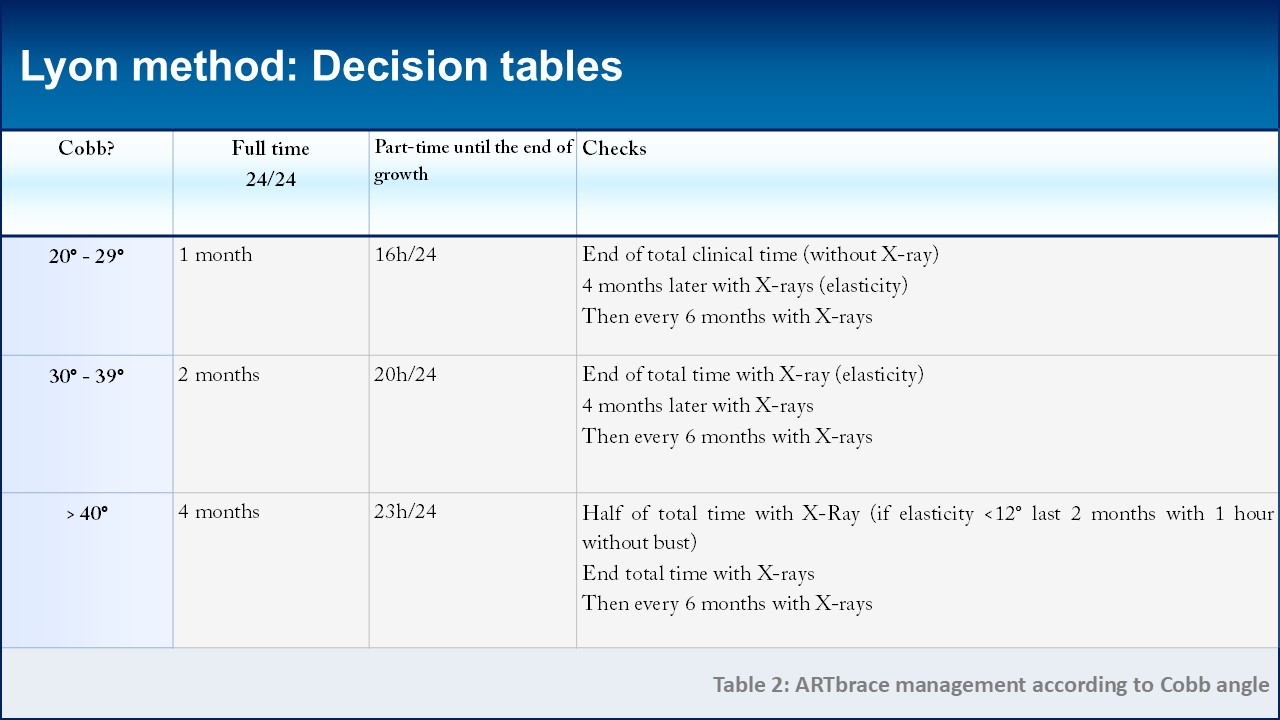 |
In instances where the use of a brace is recommended, the Lyon method distinguishes between full-time and part-time usage. Full-time brace wear replaces the previous period of plaster casting and is essential for inducing plastic deformation in the paravertebral ligament structures. The duration of full-time wear can range from one to four months, contingent upon the initial Cobb angle. Similarly, the initial prescription for part-time brace wear is based on the Cobb angulation, with further adjustments made according to the curvature's reducibility and elasticity. Reducibility is defined as the variation between the initial angulation and the angulation experienced while wearing the brace, typically averaging at 70% for the ARTbrace. When a curvature displays lower reducibility, this suggests a greater rigidity, thereby requiring an extension in partial wearing time. Elasticity, on the other hand, is calculated as the difference between the in-brace angle and the angle observed after at least one hour without the brace. On average, elasticity is recorded at 12°. Should the elasticity exceed 12°, an increase in the duration of brace wear may be warranted. |
 |
As growth reaches its conclusion, the process of removal will occur incrementally, with variations depending on the initial Cobb angle. The duration of weaning is extended by an additional four hours each day, approximately every six months, until such time that the angle stabilizes to a stable degree. In the final stage, usage is restricted to nighttime only. This gradual reduction will be carried out over a span of one to two years. Assessing bone mass during late adolescence presents challenges. A large deformation in the apical vertebra signifies insufficient resistance. When the back is flat, mechanical stress intensifies at the curve's apex. It is imperative to exercise caution while sitting, as the mechanical pressures shift to the posterior arch. Furthermore, the strength and condition of the musculature play a critical role in safeguarding the vertebral body. |
 |
The strength and quality of musculature are influenced not only by physiotherapy but also significantly by engaging in sports activities. Since the inception of the Lyon Method, there has been a harmonious integration of sports and physiotherapy. Part-time treatment acknowledges the role of sports, equating it to the function of wearing a brace. Just as a brace supports the vertebral body, muscle activity provides a protective effect. In the realm of the extrapyramidal postural system, sports foster a sense of anticipation, whereas physiotherapy enhances postural feedback mechanisms. A prevalent theory among many researchers is that a contributing factor to scoliosis is the delayed maturation of the postural system. Consequently, it is crucial to consider the age of the patient when recommending sporting activities that stimulate the postural system. Likewise, physiotherapy exercises should be adapted as the child grows and continues into adulthood, ensuring they complement the sports activities. |
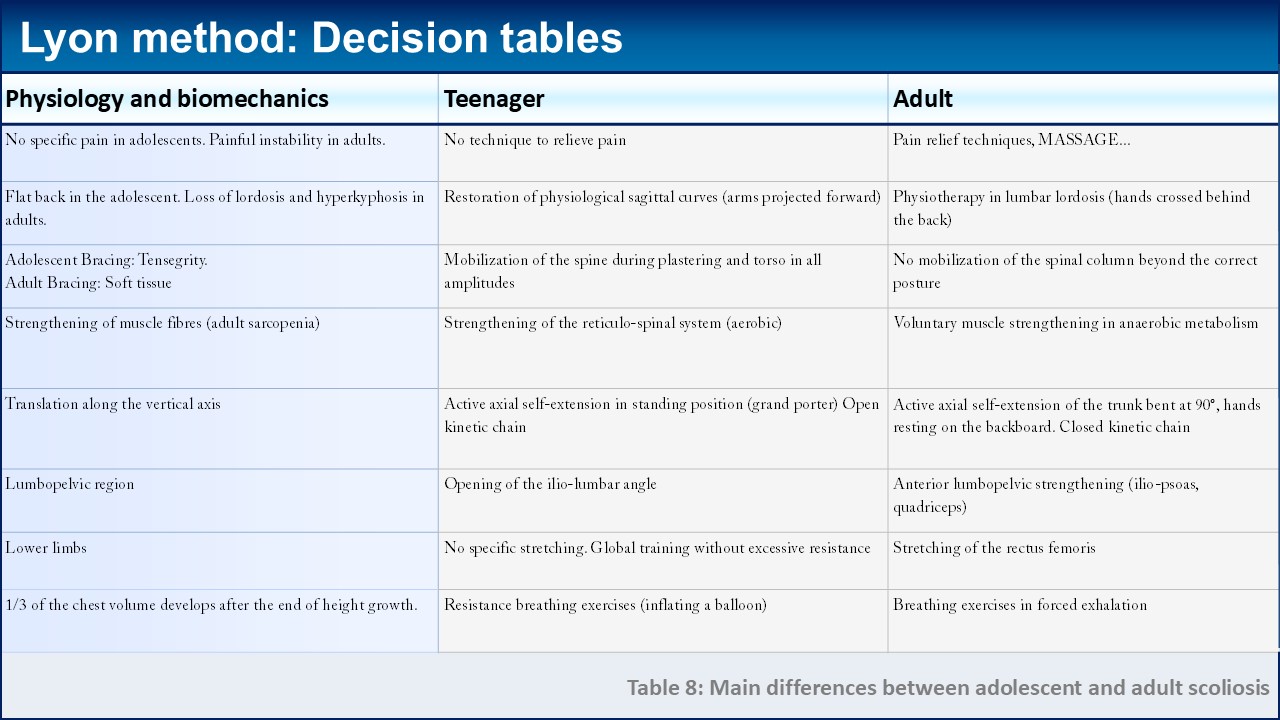 |
While it is true that most individuals undergoing treatment are adolescents, the extension and enhancement of adult life expectancy necessitate addressing scoliosis even after the growth phase has concluded. The progression of scoliosis, as revealed by its natural history, continues into adulthood, frequently resulting in pain and, notably, experiencing a phase of instability post the age of 45. The application of non-surgical conservative treatments must be tailored to align with the physiological and biomechanical principles of upright walking. This table provides a concise comparison, highlighting the primary distinctions between the growth phase and adulthood. During the growth period, flat backs are prevalent, whereas adulthood is marked by pelvic retroversion accompanied by a loss of lordosis and the presence of osteoporotic high thoracic kyphosis. The concept of tensegrity, aimed at achieving the most corrected posture, tends to diminish beyond the age of 45. Prior to the age of 40, there is no deficiency in pyramidal muscle strength, and the need to enhance muscles for anaerobic metabolism becomes particularly relevant for those over 40. |
 |
Adult scoliosis can be categorized into three distinct groups. Firstly, there is the ASA group, which comprises cases where adolescent scoliosis persists and progresses into adulthood. Secondly, we have the DDS group, representing adult-onset scoliosis often referred to as "de novo" scoliosis. This type of scoliosis typically manifests instability around the age of 55, which is later than when issues arise in the ASA group. The thoraco-lumbar and lumbar curves in DDS are shorter in length, yet they exhibit greater progression compared to ASA scoliosis. Finally, the ASD group is characterized by scoliosis that stems from muscular imbalances. Here, alongside degenerative changes that may result in a narrowing of the lumbar canal, there is also a noticeable atrophy of type I extrapyramidal muscle fibers. These fibers are predominantly found in the deep extensor muscles, which, due to their weakened state, fail to provide adequate support to the spine. |
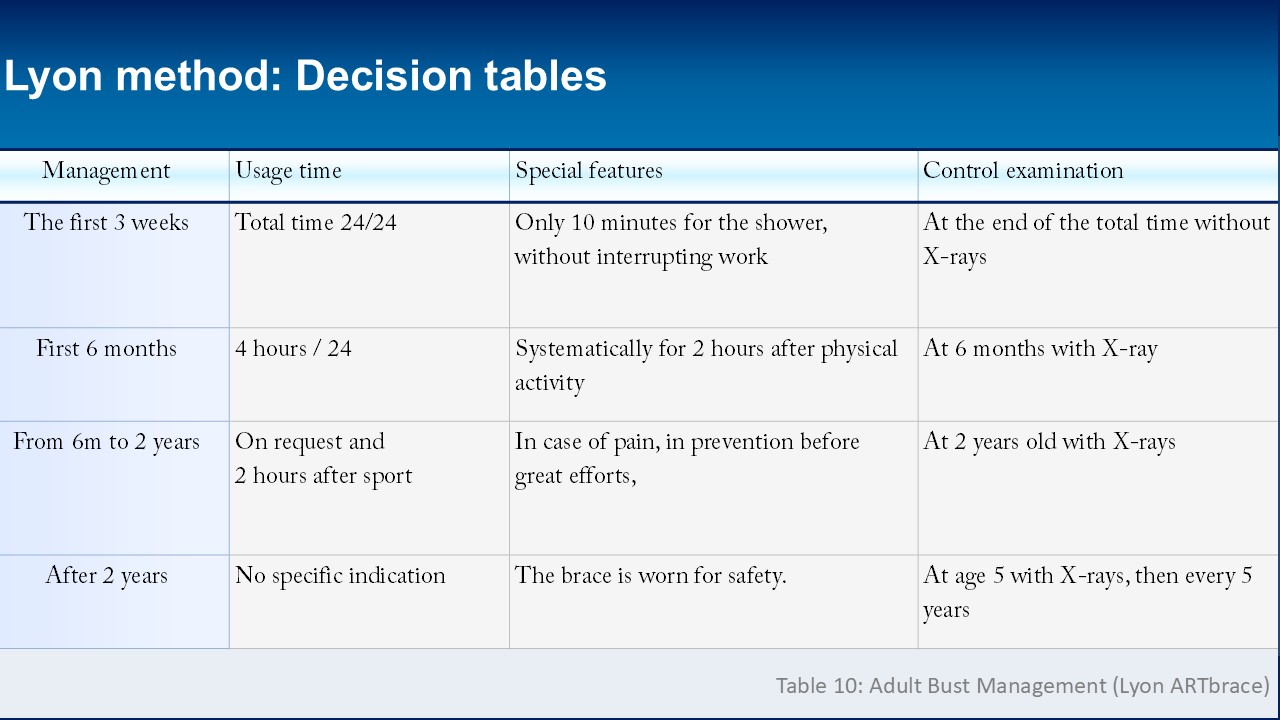 |
The utilization of braces is primarily indicated during the phase of instability or when the spinal curvature progresses by more than 2° annually over a span of five years. In cases where the curve is reversible, an adult ARTbrace corrective brace can be applied. The treatment must be continued for a minimum of six months. For plastic deformities, a complete initial treatment phase is essential to aid in initial adaptation and to verify the mechanical origin of the pain. Following this, patients typically transition to wearing the brace part-time for about six hours daily, including a regular two-hour session post-exercise. After the initial six-month period, brace usage becomes as-needed, and by the two-year follow-up mark, around half of the patients have ceased using the brace entirely. To maintain the therapeutic outcomes, physiotherapy coupled with a healthy lifestyle should be pursued alongside stabilization efforts. |
 |
The outlook for scoliosis in adults is more significantly influenced by the sagittal plane of function rather than the frontal plane. This progression is typical even in the absence of scoliosis. However, scoliosis adds complexity to this natural evolution through interconnected coupled movements. The deterioration tends to occur progressively from the lower to the upper regions. Between the ages of 20 and 40, a prominent characteristic is the reduction of lordosis. Retroversion is often enhanced by prolonged sitting, the strengthening of abdominal muscles, and the gradual compression of the intervertebral discs. During the ages of 40 to 55, there exists a risk of uneven disc deterioration, which can lead to instability and the stiffening of the spinal curve. Beyond the age of 70, osteoporosis may result in pronounced thoracic kyphosis. Muscle imbalances along with narrowing of the spinal canal frequently pose significant complications. |
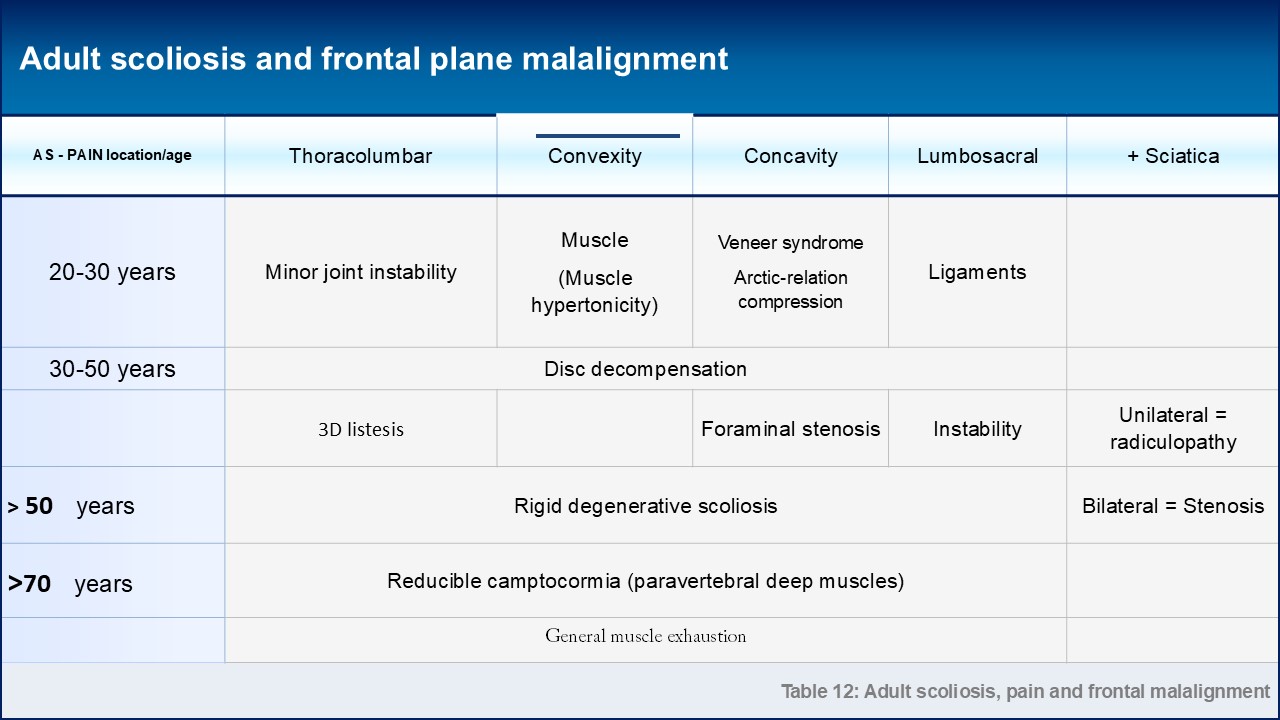 |
Experiencing pain in adulthood is the most common reason people seek medical advice. The nature of this discomfort tends to shift as one ages. For individuals between 20 and 30 years, the pain often manifests around the thoraco-lumbar region, frequently resembling minor intervertebral derangements. Osteopathic manipulation is effective in restoring mobility in such cases. At the convexity point, muscle-related pain is typically addressed through physiotherapy. For those aged 30 to 50, the pain often originates from disc issues, with rapid degeneration that can result in radiculopathy due to concavity and a frontal imbalance, especially when rigidity fails to uphold vertical posture. As people progress into their 50s to 70s, bilateral sciatica might indicate a narrowing of the spinal canal. Beyond the age of 70, conditions such as camptocormia, which affects the sagittal plane, are often discussed. Similarly, in the frontal plane, the same weakening of the extensor muscles can lead to what is known as Pisa syndrome. |
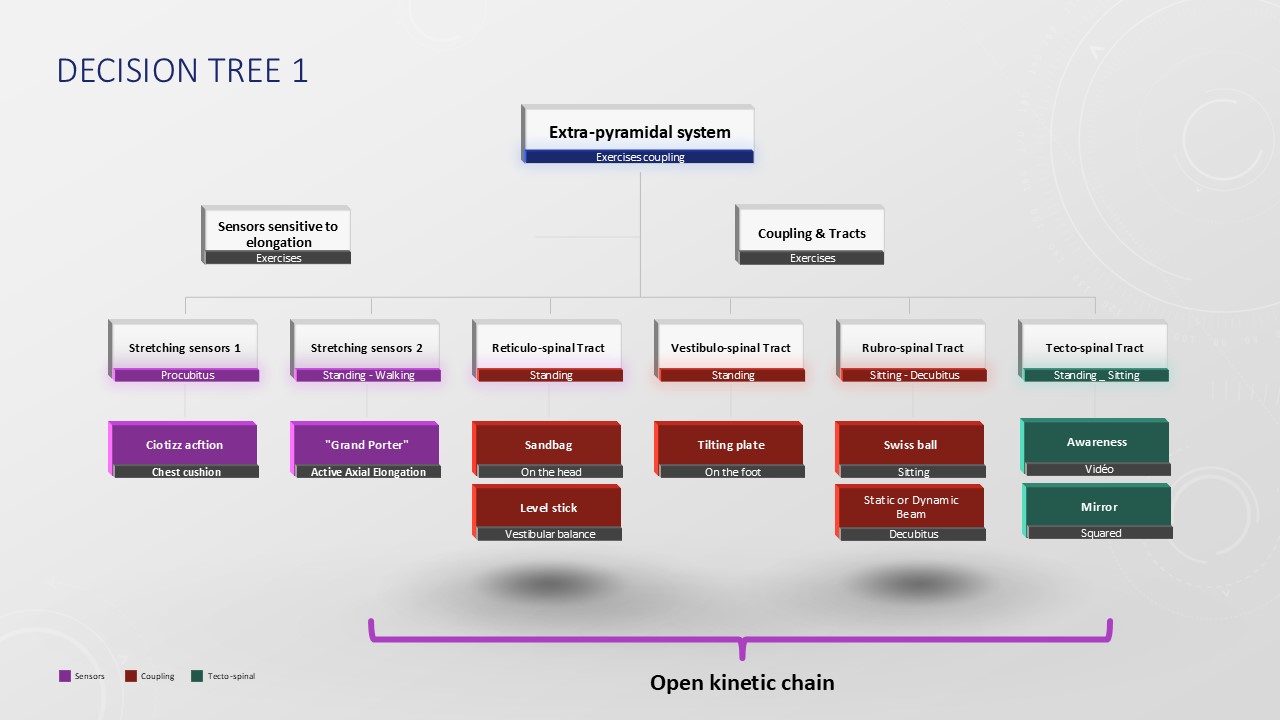 |
The Lyon Method of physiotherapy is intricately designed around the extrapyramidal postural system. This system's static and dynamic receptors are highly responsive to stretching stimuli. Techniques such as flat-back kyphotization and active axial self-elongation serve to activate these receptors effectively. Within the framework of braces, exercise number 10 employs ballistic stretching on a Swiss ball, which aids in recalibrating the corrected posture. The extrapyramidal system itself is composed of four tracts, each of which can be activated both statically and dynamically, and interestingly, they can be stimulated independently. For instance, the reticulo-spinal tract is engaged by balancing a small sandbag atop the head while maintaining an upright stance. Meanwhile, the vestibulo-spinal tract is activated through the use of tilting trays. In contrast, the rubrospinal tract is stimulated by experiencing significant imbalances while positioned on a Swiss ball. Lastly, the tecto-spinal tract is influenced through the employment of an osteopathic mirror, typically around the age of nine. |
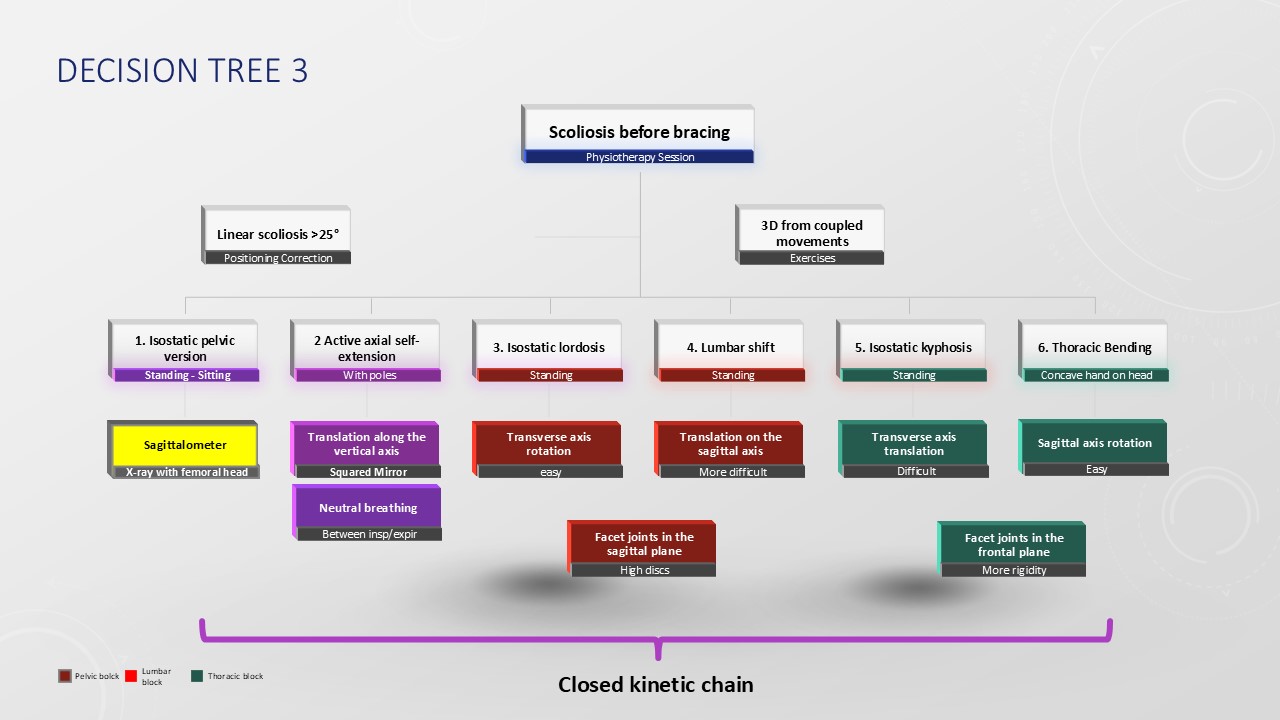 |
Physiotherapy is the primary treatment recommendation for scoliosis during the growth phase. When the curvature is less than 20 degrees, the Lyon Method focuses on activating the extrapyramidal postural system. However, for curvatures exceeding 20 degrees, mechanical correction becomes necessary, starting in the sagittal plane. To determine the optimal position for isostatic balance, a sagittalometer is employed, though the patient's actual posture might vary and will inform the specific physiotherapy approach. One of the fundamental exercises employed is active axial elongation, which can be executed in a closed kinetic chain particularly when the back maintains a flat alignment. Correcting lordosis is intricately linked with adjustments in pelvic tilt. Physiological lordosis has the benefit of promoting derotation, facilitated by asymmetrical contact at the level of the transverse convexity. In addressing the frontal plane below vertebra T10, a soft tissue transfer or"Lyon shift" is executed to realign the apical vertebra along the midline. When dealing with the thoracic level on the frontal plane, the Lyon Method advocates for flexion, which is supported by the orientation of the facet joints. This flexion advantageously opens up the concavity. |
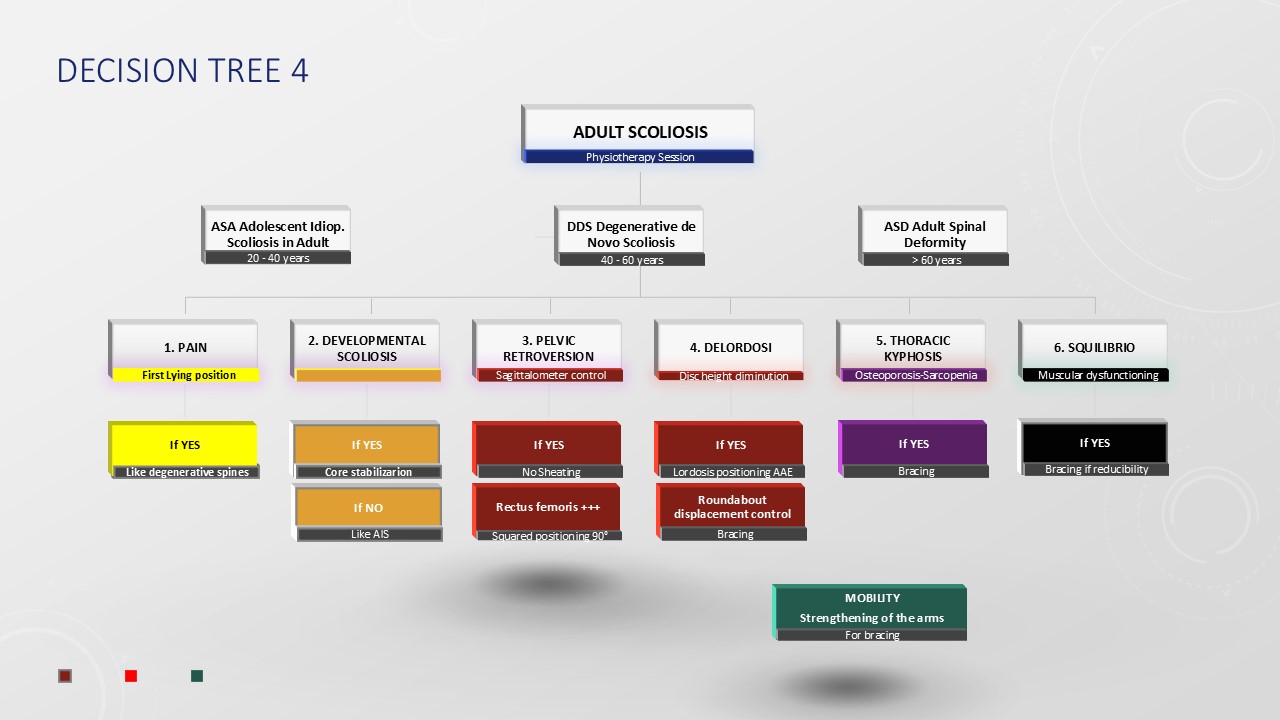 |
When assessing adult scoliosis, the age of the patient at the initial consultation serves as a crucial indicator of the scoliosis type. For individuals under the age of 50, scoliosis often represents the progression of adolescent scoliosis. Conversely, beyond the age of 50, de novo scoliosis tends to be more prevalent. Once a patient reaches the age of 70, significant imbalances, such as camptocormia or Pisa syndrome, may necessitate the use of a walker. Our analysis has categorized pain based on age and its location within the body. The progression of angular deviation can be mitigated by core exercises conducted in both the frontal and sagittal planes. Engaging in fitness routines that bolster the abdominals and gluteal muscles promotes pelvic retroversion, while physiotherapy targeting the quadriceps rectus femoris enhances anteversion. It is advisable to refrain from sports activities that induce lordosis, and instead, focus on adjusting one's sitting posture at a computer to minimize strain. Osteoporotic high thoracic kyphosis can lead to a forward shift in the center of gravity. Therefore, exercises should be practiced in a closed kinetic chain, with the hips flexed at a 90-degree angle. |
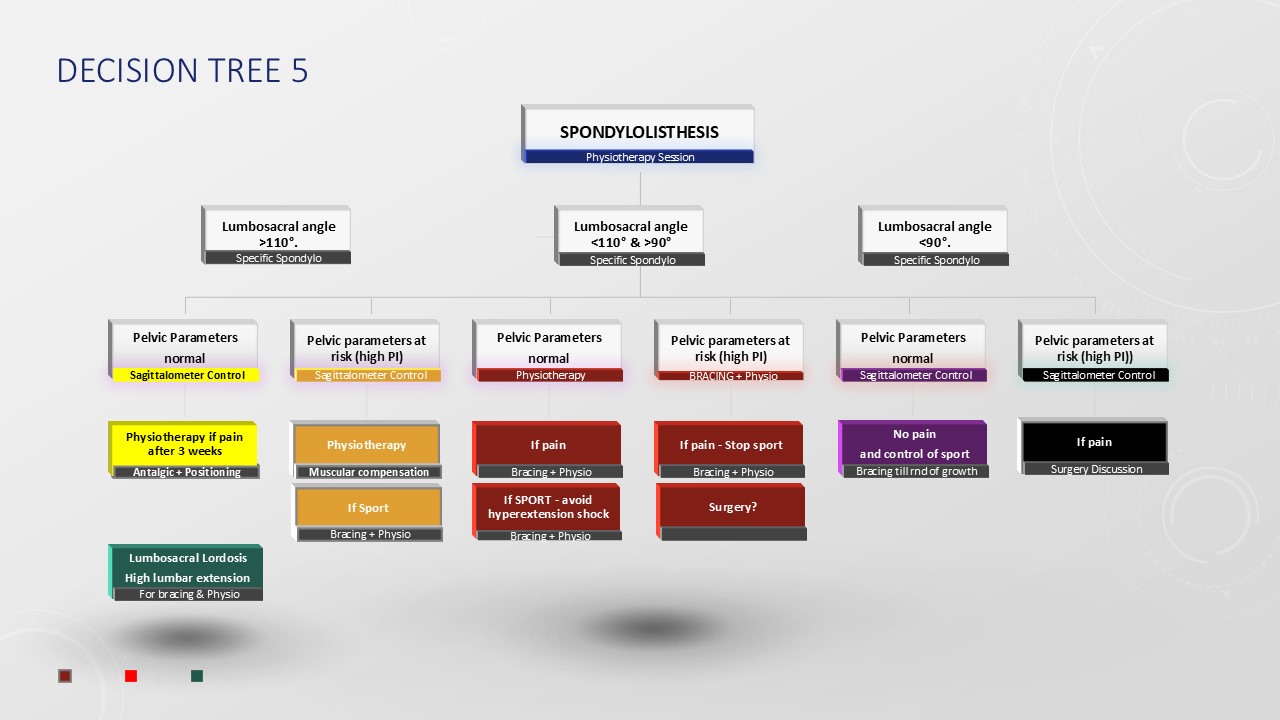 |
Spondylolysis, which affects approximately 7% of the Caucasian population, is linked to 20% of cases of lumbar scoliosis. Meanwhile, spondylolisthesis is present in 2% of population found in academic publications. Importantly, this condition is never congenital. The lumbosacral angle stands out as a vital predictive factor; when this angle exceeds 110°, the outlook is generally positive. In such scenarios, wearing a brace during the growth phase is only recommended if persistent pain is not alleviated by physiotherapy. For individuals with a high pelvic incidence, it is advisable to refrain from participating in sports that involve hyperextension. Conversely, if the lumbosacral angle ranges between 90° and 110°, the sacrum tends to verticalize, increasing the risk of condition progression. Although lumbosacral parameters might appear normal in these cases, activities involving hyperextension shocks must be strictly avoided. An increased pelvic incidence accompanied by pain necessitates conservative orthopedic management during growth. Should the lumbosacral angle fall below 90°, a significant risk of progression exists, warranting the obligatory use of a brace throughout the growth period. |
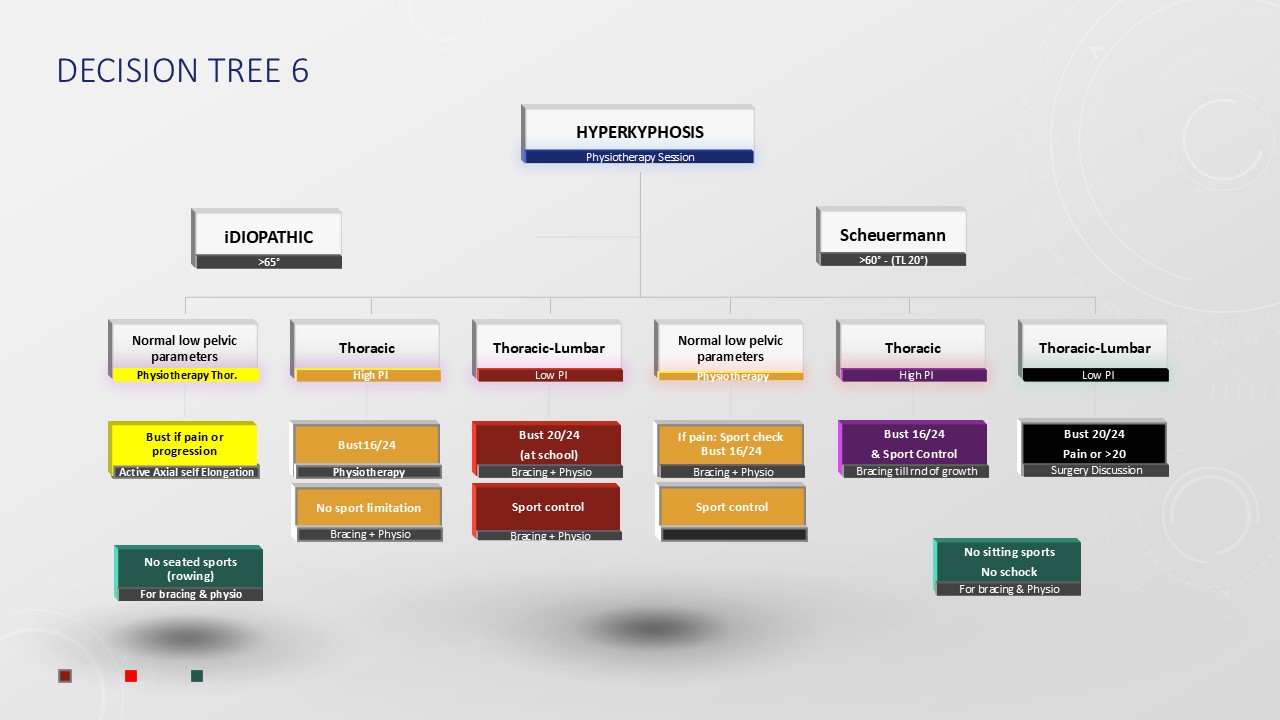 |
Thoracic Hyperkyphosis is a condition that is less prevalent than idiopathic scoliosis. Typically, it becomes painful when associated with Scheuermann’s disease. Like scoliosis, it can also present as idiopathic. Although lumbopelvic parameters are examined, their correlation with pelvic incidence holds less significance compared to lordosis. When these parameters are within normal limits, physiotherapy is usually sufficient to manage pain, thanks to the viscoplastic properties of the fascia attaching to the posterior arch and the common anterior vertebral ligament. A medium thoracic kyphosis often correlates with a high pelvic incidence, while a thoracolumbar location tends to indicate a lower incidence. In such circumstances, there might be a need for an ergonomic seat adjustment. In cases involving Scheuermann’s disease, the presence of rigidity with partial reducibility during the extension test may require the implementation of a brace. This is particularly important until the completion of growth, especially in instances of a thoracolumbar form. The protocol for using the brace will be tailored to the specific degree of kyphosis and rigidity present. |
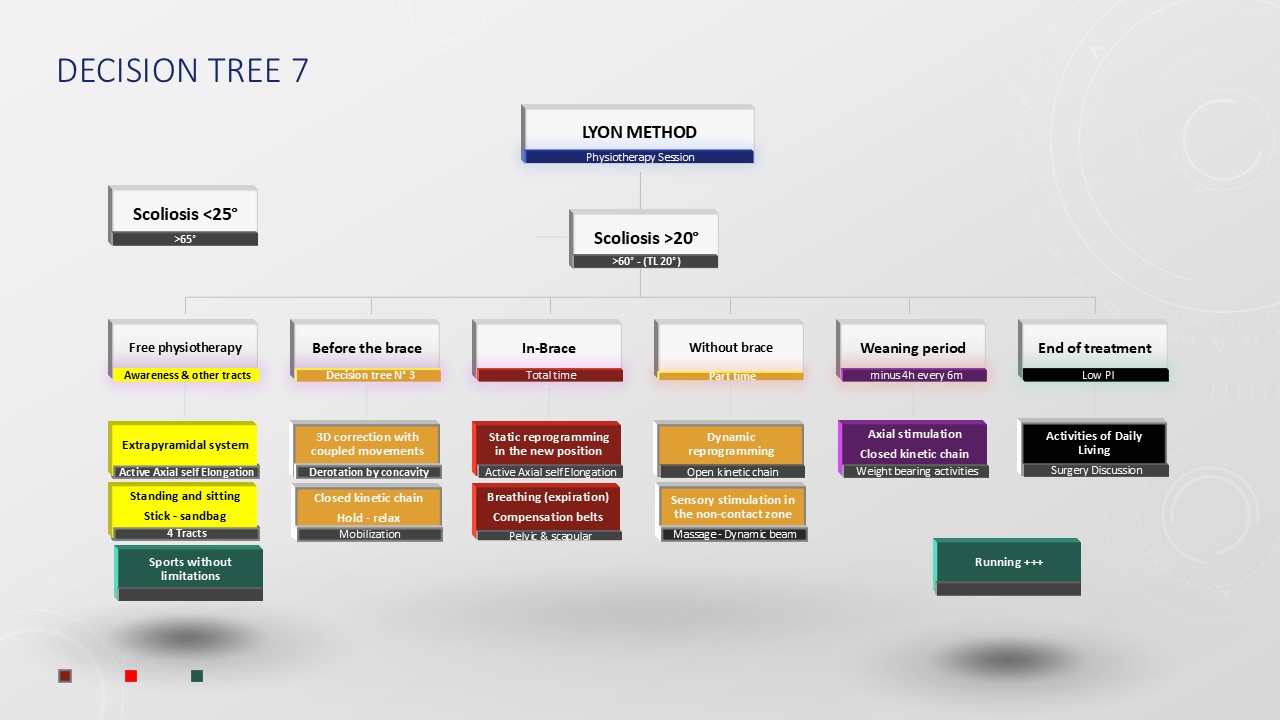 |
In the Lyon Method, scoliosis physiotherapy is complementary to brace therapy. For angulations of less than 20°, it is limited to stimulating the extrapyramidal postural system via its 4 tracts. It is adapted to the maturation stage of the postural system. When the angulation exceeds 25°, mechanical scoliosis correction exercises must complement basic physiotherapy. As with braces, these are performed using detorsion. Geometrical detorsion using axial elongation (exercise 6) and mechanical detorsion using coupled movements in the frontal and sagittal planes (exercise 7 & 8). The aim is to prepare the 3 corrections for moulding the ARTbrace. During full time, the emphasis is on exercises 9 & 10 with “grand porter” and ballistic stretching. During part-time treatment, physiotherapy is usually performed without the brace, and exercise 11 will check that the corrected position is maintained during imbalances. When the brace is removed, the emphasis is on exercise 12, which strengthens the axial muscles. To promote bone mass, sporting activities with axial impact encourage calcium fixation on the vertebral body. |
 |
The Lyon Method has long embraced the inclusion of sporting activities due to their ability to stimulate the anticipatory responses of the postural system, contrasting with physiotherapy, which primarily functions through feedback mechanisms. When the spine curvature is under 25 degrees, there are no limitations on engaging in sports. However, if the curvature exceeds 25 degrees, it becomes advisable to refrain from movements involving both flexion and rotation, as well as from rapid, extreme ranges of motion. As children grow, physical activities should be aligned with the maturation of their postural system. For those under the age of seven, encouraging activities that engage the upper body, such as those found in public parks, is beneficial. From ages seven to eleven, children often gravitate towards a preferred sport, and engaging in asymmetrical activities like tennis is not discouraged. During the period of pubertal growth, participating in sports that emphasize symmetry and flexibility can enhance Tensegrity. As growth concludes and before the stabilization of bone mass, engaging in activities with axial impact has been advocated. In adulthood, focus shifts to strengthening spiral chains in a standing position while preserving a natural lumbar curve. For individuals over 50, Nordic walking with poles serves as an excellent way to counterbalance the decline in foot proprioception. |
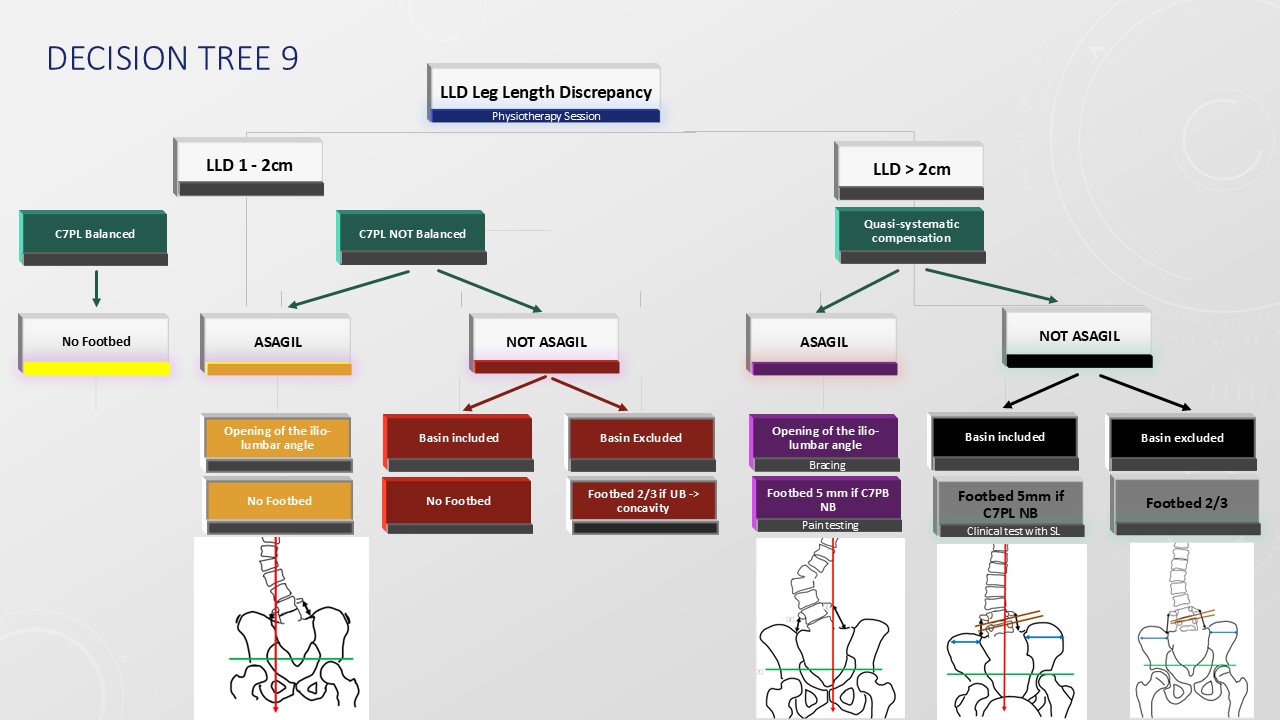 |
During the era when poliomyelitic scoliosis was prevalent, it was common to observe pelvic imbalance caused by a disparity in the lengths of the lower limbs. At that time, surgical procedures such as epiphysiodesis and limb lengthening were more frequently indicated. In contemporary practice, a routine recommendation is to employ a two-thirds compensation approach for limb length discrepancies exceeding 2 centimeters but not surpassing 4 centimeters, utilizing insole within the shoe and heel lifts. Should the discrepancy be less than 1 centimeter, no corrective measures are advised. For differences between 1 and 2 centimeters, compensation is not recommended prior to the pubertal growth spurt, as early intervention might hinder the body's natural ability to adjust, given that the growth plate on the shorter side is likely to be more active. During puberty, it is important to assess whether compensatory measures alleviate any curvature observed during the Adams forward bend test or correct potential frontal imbalances of the occipital axis. In cases where there is a tilt of the L4 vertebra, it is advisable to employ minimal compensation to facilitate the widening of the ilio-lumbar angle, particularly when the pelvis is already inclined. |
CONCLUSION |
Too much information kills information. Just like in a car, a dashboard is an operational and strategic management tool that brings together the information needed to make decisions. The dashboard complements traditional descriptive texts. The visual presentation is synthetic and well-balanced, designed to help you make the right decisions quickly. The 17 charts presented in this video are the basis of the Lyon Method's non-artificial intelligence. |
 |

